Clinical features
|
Symptoms
|
Pain
|
Pelvic examination
|
Tenderness
| |
Nodularities
| ||
Fixed retroverted uterus
| ||
Adnexal masses
| ||
Investigation
|
Ultrasound
|
Ovarian endometrioma / chocolate cyst
|
Diagnostic laparoscopy
|
Endometrial implant
| |
Biopsy
|
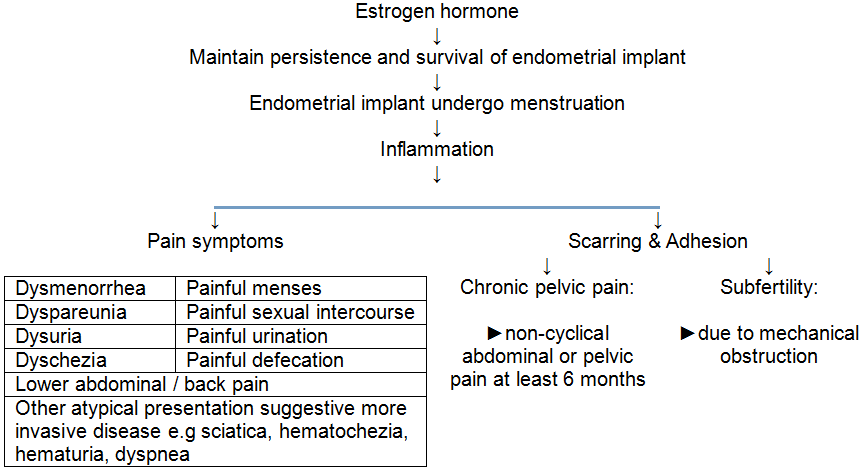
Women with endometriosis commonly presented with pain symptoms (dysmenorrhea, dyspareunia, dysuria, dyschezia, abdominal pain, back pain) eventhough some of them may be asymptomatic and only found out incidentally during surgery for other condition.
Pelvic examination may elicit tenderness which can be ill-localized or focal tenderness for example over the posterior fornix or anterior vaginal wall. Nodularities may be appreciated during pelvic examination upon palpation of the uterosacral ligament or upon rectovaginal examination, which may suggest endometrial lesions over the uterosacral ligament and the rectovaginal septum respectively. Adnexal masses found during pelvic examination of a woman with suspected endometriosis may suggest presence of ovarian endometrioma (chocolate cyst). Bimanual examination may revealed fixed retroverted uterus which suggest significant degree of adhesion has occurs.
 |
| Pelvic examination - bimanual examination |
 |
| Pelvic examination - rectovaginal examination |
Ultrasound imaging in endometriosis may revealed ovarian endometrioma / chocolate cyst which can be described as homogenous hypoechoic grain-like lesion surrounding by well defined thickened cyst wall.
 |
| Ultrasound |
Diagnostic laparoscopic examination is the gold standard investigation in diagnosing endometriosis, which allows direct visualization of the endometriotic lesions. During the laparoscopy, usually the discovered endometriotic lesions are removed and biopsy taken and sent for histopathological examination to confirm the diagnosis.
 |
| Laparoscopic examination |
 |
| Laparoscopic examination |