There are 4 procedures which have been known to have role in the management of TTTS. The procedures include: 1) serial amniotic reduction 2) microseptostomy 3) selective fetal laser photocoagulation and 4) fetal cord occlusion / coagulation.
Amnioreduction
Amnioreduction is a procedure whereby a large volume of amniotic fluid is removed from the amniotic sac by amniocentesis procedure. A needle is introduced into the amniotic sac percutaneously through the abdomen into the amniotic sac of the recipient twin who develops polyhydramnios. The aim of amnioreduction in TTTS is to control polyhydramnios in hope of prolonging the pregnancy to reduce the risk of extreme prematurity. In addition to that, amnioreduction improves utero-placental blood flow, most likely by reducing intrauterine pressure. However, the procedure doesn’t treat the cause of the disease. The effect of amnioreduction is only temporary and the polyhydramnios may develop again as the disease progress. In order to be effective, the procedure need to be done repeatedly - ‘serial amnioreduction’. Since it is an invasive procedure, it poses risk of infection towards the pregnancy. The risk of intrauterine infection is increase with the number of repeated invasive procedure done.
Amnioreduction
Amnioreduction is a procedure whereby a large volume of amniotic fluid is removed from the amniotic sac by amniocentesis procedure. A needle is introduced into the amniotic sac percutaneously through the abdomen into the amniotic sac of the recipient twin who develops polyhydramnios. The aim of amnioreduction in TTTS is to control polyhydramnios in hope of prolonging the pregnancy to reduce the risk of extreme prematurity. In addition to that, amnioreduction improves utero-placental blood flow, most likely by reducing intrauterine pressure. However, the procedure doesn’t treat the cause of the disease. The effect of amnioreduction is only temporary and the polyhydramnios may develop again as the disease progress. In order to be effective, the procedure need to be done repeatedly - ‘serial amnioreduction’. Since it is an invasive procedure, it poses risk of infection towards the pregnancy. The risk of intrauterine infection is increase with the number of repeated invasive procedure done.
 |
| amnioreduction done by amniocentesis |
Microseptostomy
It is done by creating a small hole on the intertwine membrane. Similar to amnioreduction, the aim is to control polyhydramnios by amniotic fluid dynamic equalization between both amniotic sac of the recipient and donor twin. Unlike amnioreduction, this procedure doesn’t need to be repeated. Therefore, the risk of intrauterine infection is lowered compared to serial amnioreduction. However,there is risk of the hole become larger. If the hole get larger, instead of only the amniotic fluid able to cross the septostomy, the other structure, for example the cord, may as well cross the septostomy and this increase the risk of cord entanglement.
 |
| microseptostomy |
Fetal laser coagulation
This is the 1st procedure aims to treat the cause of the disease. Fetal laser coagulation therapy is a procedure whereby blood vessels on the intertwine membrane are occluded by laser therapy, thus arrests the shunting of blood from donor to recipient and stop the transfer of potential vasoactive mediators. Initially, the procedure include coagulation of all vessels on the intertwine membrane, including the normal vessels. This may lead to acute placental insufficiency since the normal vessels that carry nutrient and blood supply are also coagulated. After that, the procedure has been improved to selective fetal laser coagulation, whereby only the vessels that lead to unbalanced transfusion are occluded. This procedure considered as the most superior therapy for TTTS, however, it only available in selected institution and requires intensive training. Besides, in cases of the affected vessels lies deep in the membrane, it might not be detected thus fetal laser coagulation could not be done.
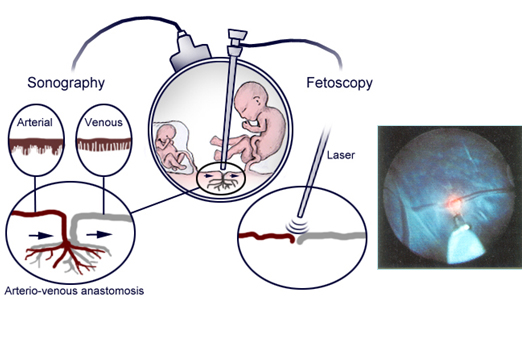 |
| fetal laser coagulation |
Fetal cord occlusion
This procedure sacrifices one twin to save the other twin. It is the final resort for cases which there is already demise or imminent demise of one of the twin. It doesn’t only stop the progression of the syndrome, but also prolonged the gestation and maximize the outcome of the other twin.
 |
| fetal cord occlusion |